
Make sure you get enough salt and minerals, please.
In “Exercise-Associated Hyponatremia” (CJASN January 2007, 2 (1) 151-161; DOI: https://doi.org/10.2215/CJN.02730806) Mitchell H. Rosner and Justin Kirven write:
“Exercise-associated hyponatremia has been described after sustained physical exertion during marathons, triathlons, and other endurance athletic events. As these events have become more popular, the incidence of serious hyponatremia has increased and associated fatalities have occurred. The pathogenesis of this condition remains incompletely understood but largely depends on excessive water intake. Furthermore, hormonal (especially abnormalities in arginine vasopressin secretion) and renal abnormalities in water handling that predispose individuals to the development of severe, life-threatening hyponatremia may be present. This review focuses on the epidemiology, pathogenesis, and therapy of exercise-associated hyponatremia.
“Severe and potentially life-threatening hyponatremia can occur during exercise, particularly in athletes who participate in endurance events such as marathons (42.2 km), triathlons (3.8 km of swim, 180 km of cycling, and 42.2 km of running), and ultradistance (100 km) races. In fact, hyponatremia has been stated to be one of the most common medical complications of long-distance racing and is an important cause of race-related fatalities (1). On the basis of recent studies of the incidence and risk factors of hyponatremia in endurance athletes, along with well-publicized reports of fatalities as a result of hyponatremia, medical directors and marathon organizations have begun to warn participants of the dangers of hyponatremia and excessive fluid intake (2).
“Exercise-associated hyponatremia (EAH) first was described in Durban, South Africa, in 1981; subsequently, Noakes et al. (3) in 1985 described the occurrence of severe hyponatremia in four athletes who participated in endurance events that were longer than 7 h. This report was followed by a similar paper by Frizzel et al. (4) that described the development of EAH in two of the authors. Importantly, before 1981, athletes were advised to avoid drinking during exercise, leading to the development of hypernatremia and dehydration in some athletes (5). Since that time, it generally has been advised that athletes consume as much fluid as possible during exercise, and rates of fluid intake during running races vary widely from 400 to 1500 ml/h or greater (6–8). In fact, most race organizers currently provide copious supplies of water and “sports beverages” throughout the race course to fend off dehydration. Concomitant with these recommendations, the incidence of hyponatremia in athletes seems to be increasing, especially in the United States (1,9–13). As the popularity of marathon races and other endurance events increase, more athletes are likely to be at risk for the development of EAH.”
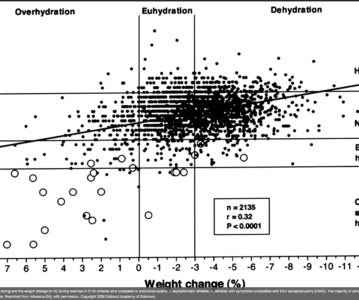
And they include a beautiful graph in their paper:

They say: “Relationship between serum sodium after racing and the weight change (in %) during exercise in 2135 athletes who competed in endurance events. •, asymptomatic athletes; ○, athletes with symptoms compatible with EAH encephalopathy (EAHE). The majority of athletes who develop clinically significant hyponatremia have positive weight changes. Reprinted from reference (34), with permission. Copyright 2005 National Academy of Sciences.”